Our pioneering, FDA-validated, tissue-based, comprehensive genomic profiling service for all solid tumours to help guide informed, personalised treatment decisions.1-3
This website is a resource intended for New Zealand healthcare professionals who are interested in information on Foundation Medicine®. If you are a New Zealand consumer, click here. These sites are not intended to provide medical advice and/or treatment guidance.
This site is produced by Roche as a partner of Roche Foundation Medicine.
Thank you for visiting our site.
You are about to leave the site to one that is not controlled or developed by Roche Products (New Zealand) Ltd.
Roche does not endorse or control the content of any linked websites and if you click OK, you agree that Roche has no responsibility or duty to you for anything that happens to you as a result. If the linked site is outside New Zealand’s jurisdiction, the information may not be consistent with New Zealand’s legislation, advertising codes or the relevant New Zealand registered Data Sheet. Please refer to the Data Sheet or Consumer Medicine Information on the Medsafe website for product information applicable to New Zealand.
Click OK to continue.


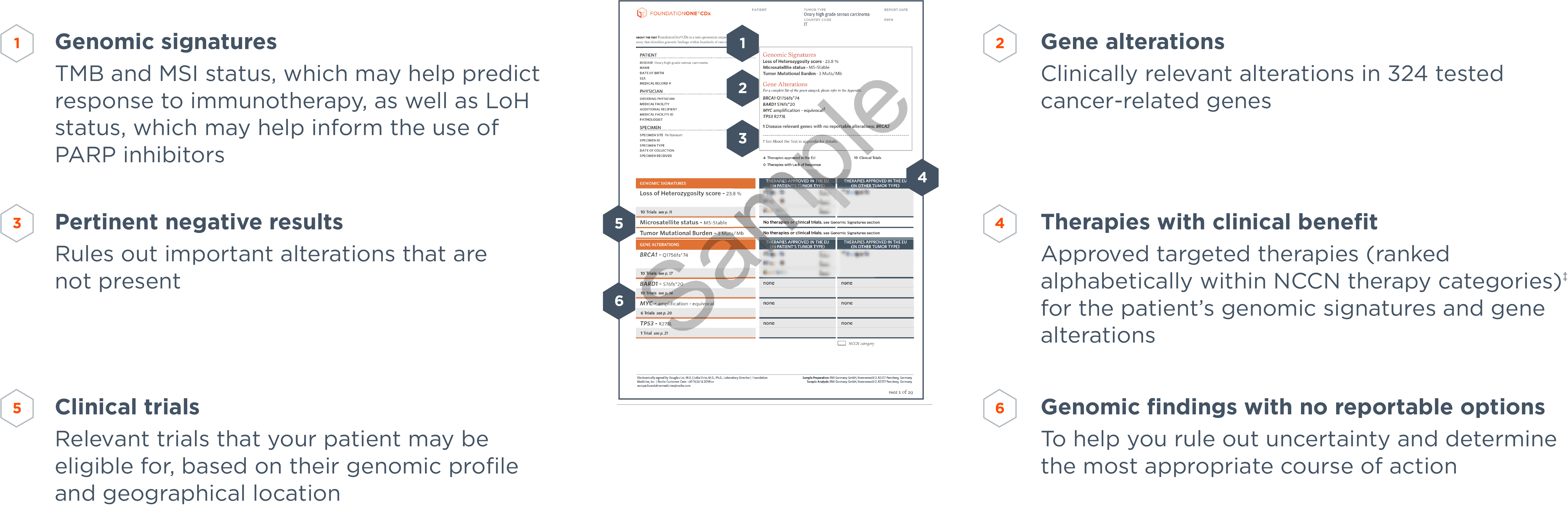
A clear, in-depth report provides insights on your patient's genomic profile as well as associated targeted therapies, immunotherapies and relevant clinical trials.5 Approved therapies are ranked alphabetically with in NCCN therapy categories.‡ The report also highlights important disease-relevant genes with no reportable alterations identified and genomic alterations associated with potential resistance to therapy to help rule out potentially ineffective treatment.5 Reports vary according to regional differences, e.g. EU reports list EU-approved therapy options to support clinical decision-making.§
When using different Foundation Medicine services across the patient journey, consistency of the reports aid comparison of the results.